Overview of Chronic Myelomonocytic Leukemia (CMML):
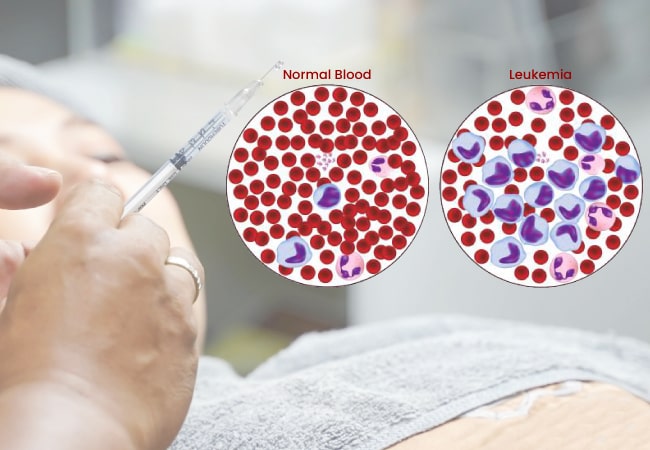
Chronic myelomonocytic leukemia or CMML is a cancer of the blood that is considered to be one of the myeloproliferative neoplasms (MPNs), a type of chronic blood cancer in which an individual’s bone marrow does not produce blood effectively. In people with CMML, their bone marrow makes excess white blood cells (monocytes). CMML should not be confused with CML, or chronic myelogenous leukemia, which is developed due to a specific genetic change known as the Philadelphia chromosome and is treated very differently.
In CMML, there is no role of the Philadelphia chromosome; instead, the disease is caused by different genetic alterations.
Diagnosis of Chronic Myelomonocytic Leukemia (CMML):
Diagnosing CMML typically involves a series of repeated tests, including blood and bone marrow tests. A clinician usually can’t confirm a diagnosis of CMML with one lab test result that indicates abnormal blood counts. Instead, a clinician will monitor an individual over a while with repeated lab tests that indicate abnormal blood counts. This is performed to rule out other diagnoses.
Bone marrow testing involves 2 steps usually performed at the same time in a doctor’s office or a hospital:
- A bone marrow aspiration to eliminate a liquid marrow sample; and
- A bone marrow biopsy is to eliminate a small amount of bone filled with marrow.
A hematopathologist evaluates the samples of the blood and marrow to confirm a diagnosis, identify the CMML subtype, and assess for damage to the chromosomes. The hematopathologist assesses the following to identify CMML:
- Persistent increased levels of monocytes in the blood
- No existence of a Philadelphia chromosome. This is assessed in a similar disease “chronic myeloid leukemia” (CML). This can be determined on behalf of the blood test looking for a specific abnormality called the BCR/ABL fusion gene.
- Less than 20% of blast cells in the blood and bone marrow
- Abnormalities in one or more types of precursor cells that develop into red blood cells (RBCs), certain types of WBC, or platelets
Other Diagnostic Tests: A doctor may order one or more tests such as those below to diagnose CMML:
- X-rays or computed tomography (CT) scans detect an enlarged spleen or liver.
- Blood and urine tests detect increased levels of lysozyme, an enzyme that exists in saliva, tears, and some immune cells like monocytes.
- Additional blood work looks for increased levels of proteins named lactate dehydrogenase (LDH) and beta 2-microglobulin, which can show tissue damage and increased white-cell production or destruction due to inflammation or certain types of cancer.
Treatment of CMML with Inqovi (decitabine and cedazuridine):
CMML can be treated with medicine Inqovi (decitabine and cedazuridine). The good news is that once your doctor has identified CMML, a proven treatment is available. Inqovi is the first and only approved oral hypomethylating agent for CMML.
Inqovi is an oral fixed-dose combination (FDC) tablet containing 35 mg of decitabine and 100 mg of cedazuridine. Cedazuridine is an inhibitor of cytidine deaminase in the gut and liver that increases systemic exposure to decitabine. Inqovi’s recommended dose is one tablet once daily on days 1 to 5 of each 28-day cycle.
References:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10528038/
https://www.cancer.org/cancer/types/chronic-myelomonocytic-leukemia.html